
Autores: Sanjay R. Patel, MD; Jessie P. Bakker, PhD; Christy J. Stitt, MS; Mark S. Aloia, PhD; and S. Mehdi Nouraie, PhD
Periódico: CHEST 2021; 159(1):382-389
DOI: https://doi.org/10.1016/j.chest.2020.07.017
Abstract
- Background: CPAP effectiveness is limited by suboptimal adherence. Prior studies of adherence have focused on middle-aged men.
- Research Question: Does CPAP adherence vary by age and sex?
- Study Design and Methods: Telemonitoring data from a CPAP manufacturer database were used to assess adherence in patients initiating CPAP therapy between November 2015 and October 2018. Analyses were restricted to patients in the United States aged 18 to 90 years.
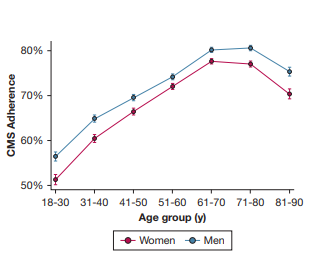
- Results: Across 789,260 patients initiated on CPAP (mean age, $55\pm14$ years; 58.2% male), overall adherence by US Centers of Medicare & Medicaid Services criteria was 72.6%, but it varied dramatically by age and sex, ranging from 51.3% in 18 to 30-year-old women to 80.6% in 71 to 80-year-old men. Patterns of use over the first 90 days demonstrated that younger age groups had peak CPAP use by the $2^{nd}$ night, with a subsequent decay in use, including abandonment of CPAP, which was greatest among 18- to 30-year-old women. In contrast, older patients steadily increase use, taking more than a week to maximize usage, and then they have much slower decays in use over time. Younger, but not older, patients have lower use of CPAP on weekends compared with weekday nights.
- Interpretation: CPAP adherence rates vary substantially by demographics, with 18- to 30-year-old women having the lowest adherence. The pattern of use over the first 90 days also varies substantially by age and sex. Further research to understand and address the causes of disparities will be crucial to maximizing the benefits of CPAP therapy.
Key Words: adherence; CPAP; disparity; sleep apnea
Abbreviations: CMS = Centers for Medicare & Medicaid Services; DME = durable medical equipment
Introduction
Obstructive sleep apnea (OSA) is a common disorder that adversely impacts sleep quality and daytime alertness as well, resulting in increased risk for motor vehicle accidents and cardiovascular disease. The most common OSA therapy, CPAP, is highly efficacious in normalizing breathing, but its effectiveness in improving health outcomes is limited by adherence. Adherence to CPAP among research participants varies from 17% to 71%. The cause of this heterogeneity is unclear, and evidence is conflicting regarding whether demographic factors such as age and sex influence adherence. A systematic review over a 20-year period reported mean CPAP usage across studies of 4.5 h/night. These data are limited in generalizability, however, because all of the CPAP users were participating in clinical research.
In 2008, the US Centers for Medicare & Medicaid Services (CMS) instituted a policy whereby long-term coverage for CPAP is denied if patients do not meet an adherence threshold of $\ge4$ hours of use on 70% of nights in a consecutive 30-day period within the first 90 days. This policy has been subsequently adopted by most private US insurers, leading durable medical equipment (DME) providers to implement widespread telemonitoring of CPAP adherence with early troubleshooting to achieve CMS adherence thresholds.
Recent data from a large clinical cohort suggest that 74.6% of patients initiated on CPAP now meet CMS adherence criteria. How adherence varies across demographic groups remains unclear. The goal of this work was to understand the distribution of adherence in a contemporary clinical population of patients initiating CPAP in the United States, including how adherence varies by age and sex.
Methods
Our sample consisted of individuals who had been registered in a large cloud-based database of CPAP therapy, Encore Anywhere (Philips Respironics). Demographic data were entered by the DME company caring for each patient. We limited our analyses to patients who began using a Philips machine between November 1, 2015 and October 31, 2018, because this is a time frame during which DME companies were regularly using Encore Anywhere to monitor all patients as standard of care. To the extent possible, we excluded those who had previously used positive airway pressure based on duplicate patient records. We limited the study population to those who were initiated on either fixed or auto-titrating CPAP, so as to prevent inclusion of patients with diseases other than OSA. We included only patients with at least 30 seconds of usage to prevent inclusion of accounts created as a demonstration or in error. We further limited the study population to patients who had a valid date of birth, sex, and zip code, and restricted to those aged 18 to 90 years and in a zip code within the 50 US states plus the District of Columbia.
A deidentified dataset was generated by Philips and transmitted to the University of Pittsburgh for statistical analysis. Because of the deidentified nature of the dataset, the University of Pittsburgh institutional review board deemed this research to be exempt from human subjects research review.
Nightly usage was used to calculate mean adherence across the first 90 days as well as to determine whether each individual met CMS adherence criteria. Dates with missing usage were input as 0 hours. A weekly trend was assessed by categorizing each day of use by day of the week. Age was categorized by decade and sex as men and women. Mean adherence levels as well as proportion meeting minimal adherence thresholds were estimated for each age and sex stratum where results were standardized to the overall sex distribution for each age stratum and to the overall age distribution for each sex.
Summary adherence data were calculated for each individual and then mixed-effects linear regression was performed to assess the impact of age and sex on mean adherence levels, where DME provider was modeled as a random effect. Similarly, mixed-effects logistic regression was used to assess the impact of age and sex on achieving CPAP adherence based on CMS criteria, with DME provider modeled as a random effect. We used the sandwich variance estimator for this random effect because it is robust to distributional assumptions. For temporal data, multilevel modeling was used to model daily usage as a function of day of the week, clustering on individual to account for within-subject correlation. Effect modification was evaluated both by assessing the magnitude of age-by-sex and age-by-day-of-week interaction terms as well as by conducting analyses stratified by age, by sex, and by day of the week.
Because the amount of missing demographic data varied greatly by DME provider, sensitivity analyses were conducted, limited to patients of those DME providers where fewer than 10% of patient accounts had missing date of birth, sex, or zip code. Given the very large sample size, we focus on effect sizes and CIs rather than P values in interpreting differences. All analyses were conducted in Stata 16.0 (StataCorp; College Station, TX).
Results
Between November 1, 2015 and October 31, 2018, 1,666,927 patients in the United States had a first CPAP account in the Encore database with at least 30 seconds of use. Of these, 161,859 accounts were excluded because of missing or out-of-range age, 521,585 because of missing sex, and 194,223 because of missing or invalid zip code. Thus, data from 789,260 patients cared for by 1,523 DME providers were included in this analysis. Mean (SD) age of this cohort was 55 (14) years, with 58.3% men. Sensitivity analyses focused on the 221,471 patients from 323 DME providers where the rate of any missing demographic data was below 10%.
Overall, mean (SD) nightly usage of CPAP at 7 days and 90 days was 4.8 (2.6) hours and 4.7 (2.6) hours, respectively. A total of 72.6% of patients met CMS adherence criteria. Among those patients cared for by DME providers with low rates of missing demographic data, the CMS adherence rate was 73.7%.
Adherence rates ranged from 80.6% in 71- to 80-year-old men to 51.3% in 18-30-year-old women. The proportion of individuals meeting CMS adherence criteria increases substantially from 54.7% in those aged 18 to 30 years to 79.0% in those aged 61 to 70 years, and then falls slightly to 73.1% in those aged 81 to 90 years. In age-standardized analyses, the proportion of women achieving CMS adherence was lower than that for men (71.3% vs 73.2%). This difference existed across ages but was more marked at younger ages. Among 51 to 60-year-olds, the absolute difference was 2.2% (72.0% in women vs 74.2% in men) but in those younger than 30 years of age, the absolute difference was 5.2% (51.3% in women vs 56.5% in men).
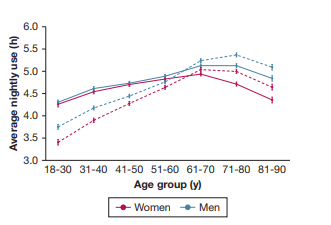
Mean hours of CPAP use also varied substantially by age and sex, with 90-day nightly average ranging from 5.4 hours in 71- to 80-year-old men to 3.4 hours in 18- to 30-year-old women. Average nightly use evolved in substantially different patterns by age and sex, going from the initial 7 days to 90 days. Both younger and older age groups had lower nightly CPAP use at 7 days compared with 61 to 70-year-olds. Over 90 days, however, the differences between 61 to 70-year-olds and older age groups diminished, suggesting that those older than age 70 take longer than a week to become fully proficient with CPAP. In contrast, the reduced usage in younger age groups at 7 days further declined over time.
In the initial 7 days, sex differences in usage were minimal up to age 60, but in older age groups, women had substantially lower CPAP use than men (4.4 h in women vs 4.8 h in men aged 81 to 90 years). By 90 days, both older women and men have improved usage, although the sex disparity persisted (mean 90-day use among 81- to 90-year-olds was 4.6 h in women vs 5.1 h in men). Among 18- to 30-year-olds, mean use at 7 days was 4.3 hours in both women and men, whereas mean use at 90 days was 3.4 hours in women vs 3.8 hours in men.
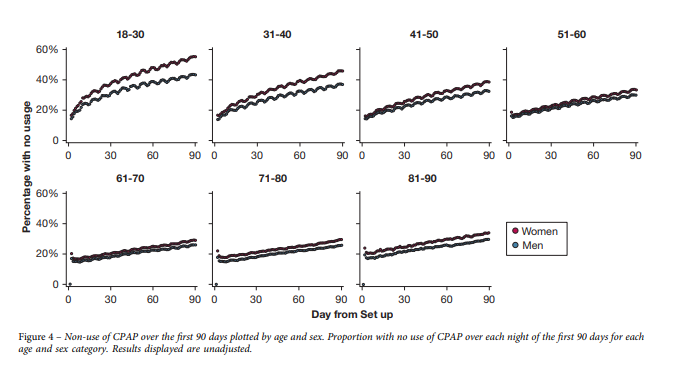
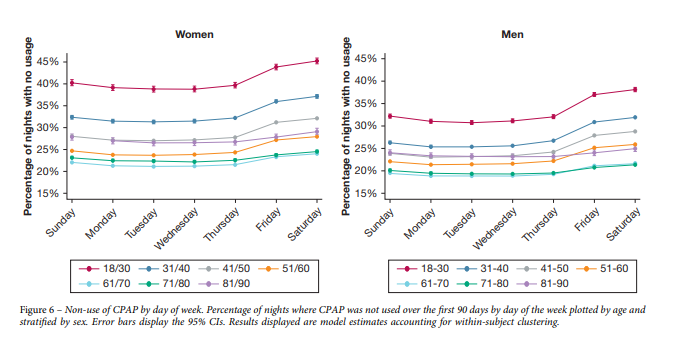
To better understand demographic differences in CPAP usage, we also explored the proportion of low adherers ($<1$ h/night), which represents people effectively abandoning CPAP. A strong U-shaped age relationship was observed in the likelihood of being a low adherer at 90 days, with the risk lowest in 61- to 70-year-olds. Young women in particular were the most likely to be low admirers (25.2% of 18 to 30-year-old women at 90 days).
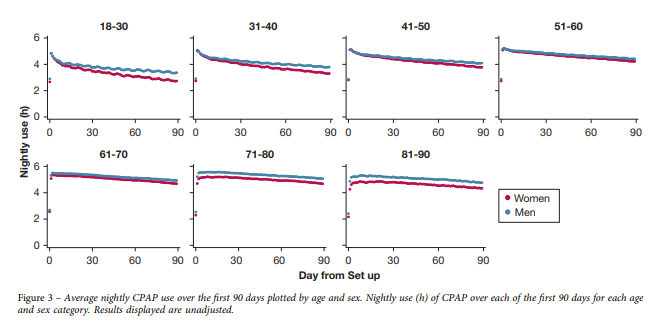
In those younger than age 60, CPAP use increases rapidly, peaking by night 2 and then decaying to give a concave contour. The most rapid decay was observed in women aged 18 to 30 years. In older age groups, CPAP use trajectory has a convex contour, increasing more gradually than in younger age groups, peaking as late as a week after initiation, and then declining much more gradually. Only 44.8% of women aged 18 to 30 years turned on their CPAP machine by day 90.
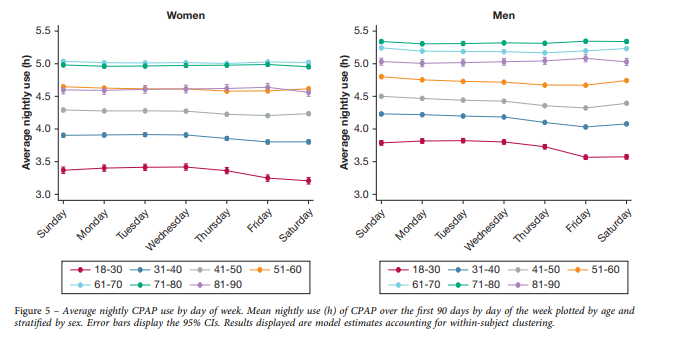
CPAP use was lower on weekends than on weeknights over the first 90 days, with highest use on Sunday nights and lowest use on Friday nights. There was virtually no variation across the week among those older than age 60 years. In contrast, among those aged 18 to 30 years, use varied from 3.7 hours on Tuesdays to 3.4 hours on Saturdays.
Discussion
Overall, in this analysis of 789,260 patient records, we found that CPAP adherence over the first 90 days varies substantially by age and sex, ranging from 51.3% in 18- to 30-year-old women up to 80.3% in 71- to 80-year-old men. Given insurance coverage policies regarding CPAP, this suggests the proportion of young women being denied long-term CPAP therapy is more than double the proportion among older men.
Younger age groups quickly achieve their maximal CPAP use by the second night but then have relatively steep declines in adherence. In contrast, older age groups take up to a week to master regular use of CPAP, after which usage remains fairly consistent over time.
One of the potential explanations for reduced usage at younger ages is the lower adherence to CPAP on weekends vs weeknights. This variability in younger patients may be related to employment, whereby retired individuals have more regular sleep schedules across the week. Potential reasons for this change include the salience attached to socializing and staying out late on weekends, sleeping away from home, and increased partner intimacy on weekends. Younger age groups are also more likely to be in less secure relationships, in which use of CPAP may be embarrassing, whereas older patients are more likely to be in stable relationships with a partner who is supportive.
In addition to age differences, we found a small but consistently reduced level of adherence in women compared with men across all ages, but this difference was magnified at extremes of age. In those younger than age 30, women have rates of use nearly identical to those of men during the first week, but their usage declines much more steeply over time, leading to abandonment. The pattern seen in those older than age 70 years was different: women had substantially reduced usage of CPAP in the first week, and this disparity remained fairly constant out to 90 days.
Societal expectations that place a greater emphasis on the appearance of women may adversely impact the decisional balance such that they are less accepting of a treatment that may be viewed as unattractive. Specific challenges related to CPAP use such as claustrophobia may also be more common in women than men. Furthermore, differences in OSA pathophysiology may explain our findings, because the OSA phenotype differs by sex, with women tending to have lower severity as assessed by the apnea-hypopnea index, but greater evidence of rapid eye movement predominant disease.
Methodological Considerations and Limitations
Our findings provide novel insights into the epidemiology of CPAP adherence by identifying demographic groups who have systematically lower adherence rates. The steep decline in CPAP use in younger patients suggests that interventions to increase motivation need to occur almost immediately after initiation in this group.
Chief among the limitations is the limited information regarding factors such as disease severity, symptoms, prior OSA treatments, race, and socioeconomic status, which all may impact CPAP adherence. Future research merging electronic health records with CPAP datasets would allow for a more comprehensive understanding of the factors associated with adherence.
In summary, short-term adherence rates to CPAP vary widely by age and sex, with the lowest rates observed in young women. Substantial differences in patterns of use are seen over the first weeks, suggesting the need for individualizing interventions to maximize adherence.
References
- Veasey SC, Rosen IM. Obstructive sleep apnea in adults. N Engl J Med. 2019;380(15):1442-1449.
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178.
- Rotenberg BW, Murariu D, Pang KP. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J Otolaryngol Head Neck Surg. 2016;45(1):43.
- Cistulli PA, Armitstead J, Pepin JL, et al. Short-term CPAP adherence in obstructive sleep apnea: a big data analysis using real world data. Sleep Med. 2019;59:114-116.
- Tripepi G, Jager KJ, Dekker FW, Zoccali C. Stratification for confounding—part 2: direct and indirect standardization. Nephron Clin Pract. 2010;116(4):c322-c325.
- Zeger SL, Liang KY. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42(1):121-130.
- Lederer DJ, Bell SC, Branson RD, et al. Control of confounding and reporting of results in causal inference studies, guidance for authors from editors of respiratory, sleep, and critical care journals. Ann Am Thorac Soc. 2019;16(1):22-28.
- Sin DD, Mayers I, Man GC, Pawluk L. Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population-based study. Chest. 2002;121(2):430-435.
- Pelletier-Fleury N, Rakotonanahary D, Fleury B. The age and other factors in the evaluation of compliance with nasal continuous positive airway pressure for obstructive sleep apnea syndrome: a Cox’s proportional hazard analysis. Sleep Med. 2001;2(3):225-232.
- Budhiraja R, Parthasarathy S, Drake CL, et al. Early CPAP use identifies subsequent adherence to CPAP therapy. Sleep. 2007;30(3):320-324.
- Woehrle H, Graml A, Weinreich G. Age- and gender-dependent adherence with continuous positive airway pressure therapy. Sleep Med. 2011;12(10):1034-1036.
- Weaver TE, Maislin G, Dinges DF, et al. Self-efficacy in sleep apnea: instrument development and patient perceptions of obstructive sleep apnea risk, treatment benefit, and volition to use continuous positive airway pressure. Sleep. 2003;26(6):727-732.
- Gentina T, Bailly S, Jounieaux F, et al. Marital quality, partner’s engagement and continuous positive airway pressure adherence in obstructive sleep apnea. Sleep Med. 2019;55:56-61.
- Morrell MJ, Finn L, McMillan A, Peppard PE. The impact of ageing and sex on the association between sleepiness and sleep disordered breathing. Eur Respir J. 2012;40(2):386-393.
- Ye L, Antonelli MT, Willis DG, Kayser K, Malhotra A, Patel SR. Couples’ experiences with continuous positive airway pressure treatment: a dyadic perspective. Sleep Health. 2017;3(5):362-367.
- Edmonds JC, Yang H, King TS, Sawyer DA, Rizzo A, Sawyer AM. Claustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apnea. Heart Lung. 2015;44(2):100-106.
- Anttalainen U, Tenhunen M, Rimpila V, et al. Prolonged partial upper airway obstruction during sleep: an underdiagnosed phenotype of sleep-disordered breathing. Eur Clin Respir J. 2016;3:31806.
- O’Connor C, Thornley KS, Hanly PJ. Gender differences in the polysomnographic features of obstructive sleep apnea. Am J Respir Crit Care Med. 2000;161(5):1465-1472.
- McArdle N, King S, Shepherd K, et al. Study of a novel APAP algorithm for the treatment of obstructive sleep apnea in women. Sleep. 2015;38(11):1775-1781.
- Guilleminault C, Quera-Salva MA, Partinen M, Jamieson A. Women and the obstructive sleep apnea syndrome. Chest. 1988;93(1):104-109.
- Redline S, Kump K, Tishler PV, Browner I, Ferrette V. Gender differences in sleep disordered breathing in a community-based sample. Am J Respir Crit Care Med. 1994;149(3 Pt 1):722-726.
- Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): description of lifestyle intervention. Diabetes Care. 2002;25(12):2165-2171.
- Pandey A, Mereddy S, Combs D, et al. Socioeconomic inequities in adherence to positive airway pressure therapy in population-level analysis. J Clin Med. 2020;9(2).
Positive airway pressure therapy and all-cause and cardiovascular mortality in people with…
Obstructive Sleep Apnea, Positive Airway Pressure, and Implications of Early Treatment in Parkinson…
Impact of Exclusive Mouth Route and Lateral Position on the Efficacy of Oronasal CPAP to Treat OSA…
Effects of Inspiratory Muscle Training on Obstructive Sleep Apnea: A Systematic Review and…
O que você achou deste conteúdo? Conte nos comentários.



